





Latch
One of the most essential aspects of breastfeeding is the attachment of the baby’s mouth to the breast of the mother. This is called the latch.
Why is latch important?
- It directly impacts the amount of milk that can be transferred from the mother’s breast into the baby’s mouth.
- It determines whether breastfeeding will be painful for the mother.
What is a good latch?
A good latch is a latch in which the baby is able to transfer milk effectively without causing any pain to the mother.
How to latch the baby onto the breast?
It’s very important that when the baby is going to latch, her mouth is wide open, and she takes not just the nipple, but as much part of the areola as possible into her mouth. There are certain steps that can be taken to ensure that the baby opens her mouth wide enough to form a deep latch.
The mother and the baby are in a comfortable position – Individually and together.
Mother’s positioning:
- The mother should not be leaning in front, should be leaning slightly back so that she is relaxed with no strain on any part of the body. Make sure that gravity is not causing the breast to come on top of the baby and making the baby uncomfortable.
- Should have pillows to make her comfortable. No floating hands/ legs. Hands can be supported by pillows and legs by a footstool if sitting on a chair and legs are floating.
- The mother could either use a pillow (breastfeeding/regular) or not use one based on whatever is comfortable for her.
Baby’s positioning:
- The baby is placed at the height of the mother. The nose of the baby at the height of the nipple. Use pillows if needed to support the baby to come to the level of the breast (normal/breastfeeding).
- No twists, the baby should be facing the mother entirely. The Baby’s neck, shoulder and hip should be on an imaginary straight axis.
- The baby’s stomach should be facing the mother’s stomach – tummy to tummy.
Mother and Baby Together:
- Baby hugging the breast hands not coming in the way of the latch by being very close to the areola, but enabling the latch with hands wide open and holding the mother as a hug (no mittens).
- There should be no space between the mother and the baby.
- The mother supports the whole spine of the baby with one hand as the baby is fully facing the mother.
- The palm of the mother holds the baby at the base of the neck – thumb on one ear and index on the opposite ear, the palm of the hand stably placed in the space between the baby’s shoulders. The baby should be able to push the head behind and unlatch itself if needed.
You can read more about positioning in detail here.
Following are the steps to latch the baby on in a Cross-Cradle Hold (the breast is held with the same hand as the breast the baby would be latched on to).
- The mother supports the spine of the baby entirely with the hand opposite to the breast that is going to be offered.
- The mother holds the breast in a ‘U’.
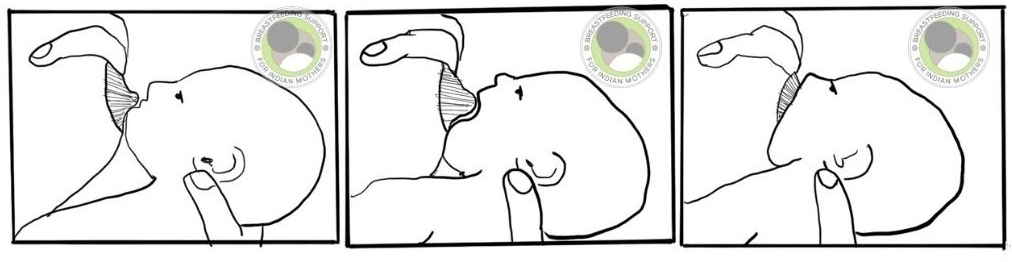
- Tickle the baby with the nipple from nose to chin/ right below the nose.
- Nipple pointing towards upper palate when the baby latches on.
- Baby opens mouth wide (about 120 degrees).
- The mother quickly guides the baby’s neck towards the breast to latch.
- The baby’s chin should not be too close to the neck, otherwise, the baby will not be able to open its mouth wide. A slight tilt away from the neck for a very small baby ideally to make sure this is not happening.
- Baby tilts/ thrusts head back to latch on to the breast.
- The baby should be brought to the breast, the mother shouldn’t move toward the baby to latch the baby on.
Characteristics of a deep latch
- It is deep. The baby takes in her mouth not only the nipple, but as much part of the areola as possible. Since the stimulation points for milk ducts are situated on the areola, it is very important that the baby takes as much of the areola as possible in her mouth. When the baby takes only the nipples, it’s called a shallow latch. In a shallow latch, there’s very less to no stimulation, leading to very less to no milk flow.
- It is asymmetrical. What is meant by this is that when a baby is latched onto the breast, her lower jaw takes more part of the areola into the mouth as compared to the upper jaw and the nipple points upwards to the back of the baby’s upper palate, not to the throat directly.
- The baby is attached to the breast slightly off-centre. More breast above the baby’s upper lips is visible as compared to lower lips. The baby’s chin will be touching the breast and the nose will be very close to it.
- The baby’s lips will be flanged outside like a fish. Both the lower and upper lip will be curled outwards, but the lower lip will be curled out more than the upper lip will be.
- It is painless. When the latch is good, breastfeeding is completely painless for the mother.
Common problems in latching
- Shallow latch: It can be OK when the child is not transferring milk, and comfort nursing. However, it can be painful and can lead to sore and cracked nipples when the child is attempting to transfer milk with a shallow latch. This can be corrected by following the latching steps diligently and by seeking professional help if sore and cracked nipples persist even after attempting a deep latch.
- Flat or inverted nipples – it can be a challenging task to latch a baby when the mother has flat or inverted nipple(s). But it is possible. The most important thing to remember here is that babies don’t latch on to the nipple. They latch on to the breast. Thus, nipple shape can be a factor, but not a deciding factor, in achieving a good latch. Using breast shells, and hand expressing/pumping right before nursing in some cases may help in releasing or elongating the nipples, making it easier for the baby to latch. Please click here if you are dealing with flat and inverted nipples.
- Edema – Many times, the mother is given Intravenous (IV) Fluid during labour. This can lead to retention of fluid even in breasts, and breasts become hard. Thus, the nipples may seem flattened and are difficult to latch on. Reverse pressure softening can help a lot in softening the area of the nipples and areola, making it easier for the baby to latch. Click here to learn more about the technique.
How to unlatch?
This is a very important yet ignored point. When a baby latches onto the breast, a vacuum is created. To unlatch the baby, this vacuum needs to be broken. If one tries to unlatch the baby by force or only by pulling the nipple out, it can be very painful for the mother and can cause injury to the nipple as well. Therefore, if and when the mother needs to unlatch the baby, it is important to break the vacuum created by suction first. This can be done by inserting one’s little/the smallest finger into the baby’s mouth from the corner of the baby’s mouth, and then tugging the corner of the baby’s mouth gently in order to break the suction. It is important to note that the finger should be clean.
Knowing the correct unlatching technique comes very handy when the mother is working on correcting the latch. Each time, the latch is shallow or painful or unsatisfactory, she can unlatch the baby to achieve a deep latch.
If you are seeking one-on-one lactation support from the comfort of your home, Breastfeeding Support for Indian Mothers offers Online Lactation Consultation, which can be booked here.
We also provide volunteer support on our 24X7 support group on Facebook, which you can join by clicking here.
P.S.: We do not accept Facebook profiles with inaccessible information. If your profile is locked/ inaccessible, you will need to send a Personal Message to our Facebook Page to join our free Facebook support group.
Wish to speak with a member of our team who is a certified lactation professional and also an experienced breastfeeding mother, click on this link.
Medical Advice Disclaimer
THIS WEBSITE DOES NOT PROVIDE MEDICAL ADVICE.
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. No material on this site is intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or other qualified health care provider with any questions you may have regarding a medical condition or treatment before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Disclaimer
We understand and acknowledge that parents and babies can be of various genders on a spectrum of LGBTQI+. Families come in diverse flavours. However, in our articles, for the sake of simplicity and convenience, we will be referring to the breastfeeding parent as the mother and using the female pronouns- ‘she’ and ‘her’ for babies. Babies can be nourished and nurtured in different ways and while we have used the terms breastfeeding and nursing, we recognize that parents can opt to chest feed or finger feed.
We don’t have conflicts of interest and declare, and we are compliant with the WHO code of marketing of breastmilk substitutes and the IMS act.
In case you find any information on this website that needs to be updated, please write to us at info@bsim.org.in